






Study design
The details of the study methods adopted for this study was published elsewhere in other article23.
A quasi-experimental study was conducted among pregnant women who were in the second trimester (gestational ages less than 16 weeks), not suffering from any chronic illness, had no severe anemia and provided verbal consent to participate in the study. Pregnant women were recruited and assigned to receive nutrition education and IFAS in the intervention group and routine antenatal care services only in the control group by two stages. The study was performed as per the principles of Helsinki Declaration.
Study setting and sampling
The study was conducted in Butajira city administration located in 135 km southern part of Ethiopia. In 2022, the population of Butajira city administration is 89, 824 and has increased by 6.8% from 2007.
The sample size was determined by using the formula for comparison of two population proportions for the intervention and control groups.
$$\:n=\frac\left(Z_1\:+\:\:Z_2)^2*\:2p\right(1-p)(P_2\:-\:P_1\:)^2\:\:\:$$
The following assumptions were considered when estimating the required minimum sample sizes: the expected proportion of pregnant women with good knowledge (P1) 0.77 and P2 was 0.5224. We wanted to detect an absolute increase of 25% in the intervention group at 5% significance level, and 80% power. The calculated sample size was multiplied by 1.5 to adjust for design effect and added 10% loss to follow up, the final sample size was 198. After assessing for eligibility, primary author randomly assigned pregnant women to the intervention and control groups in a 1:1 ratio using coin tossing (Fig. 1).
Data collection
The trained data enumerator collected data from pregnant women who gave written informed consent to participate in the study. The baseline data was collected using interviewer administered questionnaire. The questionnaires included socio-economic characteristics of women and their households, obstetric history, prenatal health seeking behavior, and measure variables relevant to maternal nutrition during pregnancy, IFA compliance level and biochemical assessment such as hemoglobin level estimation were done.
At the end of intervention, data on IFA compliance and hemoglobin status were collected. Compliance with the IFAS was assessed by pill count based on the number of remaining pills in the retained prescribed bottles. The number of unused pills in the retained pill bottles or strips was counted and recorded at the last visit following the last week of the intervention. If pregnant women were able to take at least ≥ 72 IFAS pills or 80% from the total take period, they were considered an adherent to the IFAS utilization, whereas those who were not able to take < 72 IFAS pills or < 80% from the total intake period were considered non-adherents to the IFAS intakes6.
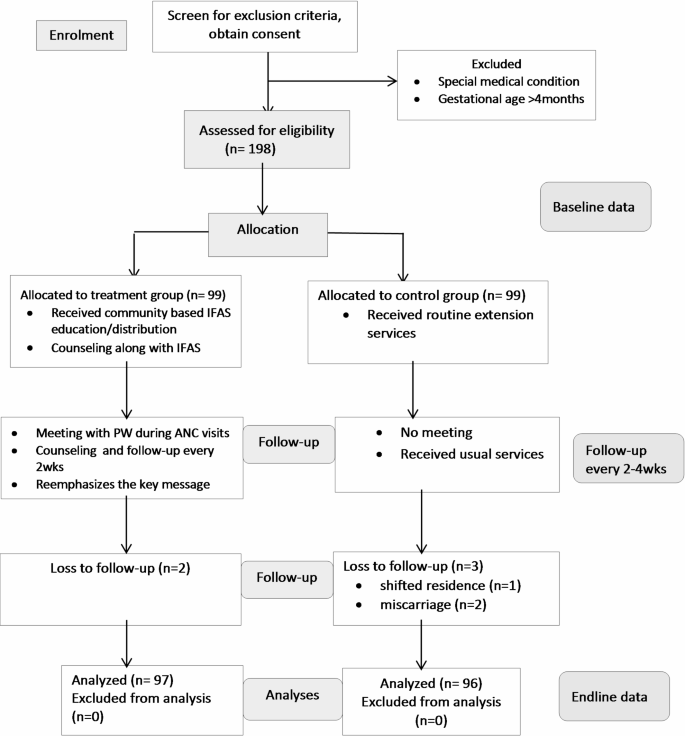
Flow diagram showing the effect of community-based nutrition education and counseling targeting knowledge and attitude towards IFAS among pregnant women.
Hemoglobin was measured using a portable and battery-operated machine (HemoCue, Angel Holm, Sweden). After swiping the site with disinfectant, a finger prick was made to obtain blood for hemoglobin measurement. The first two drops were swapped away and the third drop was used to fill the micro cuvette for reading of the hemoglobin. Maternal anemia is defined as Hemoglobin value < 11 g/dl during pregnancy25.
The intervention
Nutrition education was delivered in Amharic. An organized work schedule, counseling cards, and nutrition education were provided to the intervention group. The core messages for the lessons were generated using the health belief model (HBM)26. It was modified in the recommendation to the Ministry of Health (MOH), Ethiopia27. The messages were framed in a way that addresses all components of HBM constructs like perceived susceptibility (the belief about the likelihood of developing a health problem or experiencing negative outcomes), perceived severity (the assessment of the seriousness or consequences of a health problem), perceived benefits (the belief about the positive effects of taking action to prevent or treat a health problem), perceived barriers (the belief about the costs or obstacles of taking action), cues to action (the factors that trigger or motivate action, such as symptoms, media messages, or social influences), self-efficacy (the confidence in one’s ability to perform a health behavior successfully). The health belief model was selected because the desired behavioral change is at an individual level and due to its convenience and simplicity.
For the intervention and control groups, baseline and endline assessments were collected. Following the gathering of baseline data, intervention groups were placed in groups at nearby village and received nutrition education regularly, once every two weeks, for a period of three months (six sessions) for 30 to 45 min per session. Four nurses with Bachelor of Science (BSc) degrees delivered nutrition education, while two Master of nutrition (MSc) specialists supervised the nutrition education sessions. The core contents of the session were: increasing knowledge about iron-rich food sources, iron-folic acid supplements (IFAS) (how to take the IFAS, when to take it, and how to absorb it more, foods rich in iron and folic acid, common side effects and their management; and enhancers/inhibitors of iron/folic absorption), iodized salt, meal frequency, and portion size with increasing gestational age; food groups; taking day rest; reducing heavy workloads; enhancers and inhibitors of iron absorption; increasing utilization of health services; and interrupting the intergenerational life cycle of malnutrition; increasing pregnant women’s perceptions of undernutrition and factors leading to it; poor eating practices causing inadequate dietary intake and disease; a diet adjustment.
Nutrition education sessions included presentations, discussions, demonstrations, and picture-based exercises. Key messages, realistic activities, and the GALIDRAA (greet, ask, listen, identify, discuss, recommend, agree, and make follow-up appointments) processes were all identified by the trainers as crucial counseling abilities. After the pregnant women were enrolled, reasonable attempts were made to encourage their retention and full follow-up for the duration of the trial by providing them with incentives to reduce missing data. Periodic conversations about compliance with the intervention during routine meetings and home visits by trainers served to retain interest in the study. Moreover, home visits were planned to lessen the strain of follow-up visits among pregnant women.
Intervention fidelity
The investigators developed criteria to assess the fidelity of the intervention based on the National Institutes of Health (NIH) Behavioral Change Consortium’s best practice recommendations28. The criteria used include research design, training of nutrition educators, intervention delivery, and receipt of intervention. To balance the variations, equal numbers of eligible participants were selected for the intervention and control groups. In addition, to reduce information contamination between the intervention and control groups, non-adjacent kebeles were selected. Intervention “dose” was adequately described and the same for each group in the study, which also included a comparison group and a counseling manual. To minimize between-educators variation, educators received instruction utilizing a manual, simulated counseling sessions, and ongoing supervision. Educators’ knowledge and skills were assessed by pre- and post-training tests and practical evaluation. Implementation of the intervention was assessed using post-intervention knowledge and attitude towards IFAS. Besides, each woman received an equal number and frequency of counseling, as well as the length of contacts within an intervention group to make the process standardized.
Outcome measure
The primary outcome for this study was the effect of nutrition education and IFAS on anemia level of pregnant women after three months of intervention. Secondary outcomes included the adherence to IFAS.
Data management and analysis
The data were entered, cleaned, coded, and analyzed using Statistical Package for Social Science version 26.0 software. The characteristics of respondents were also described in both the intervention and control groups. The wealth index was computed using principal component analysis as a composite indicator of living standards based on ownership of selected household assets, size of agricultural land, number of livestock, materials used for housing construction, ownership of improved water and sanitation facilities, and household possessions5. The wealth index values were calculated by summing up the scores of sixteen components. Ultimately, three categories (low, medium, and high) were generated by splitting the wealth index values into three equal classes.
Comparisons of mean hemoglobin level between and within the control and intervention groups were done using independent and paired sample t-tests (assuming equal variance), respectively. The analysis of the effect of the intervention was done using a Difference-In-Difference (DID) (percentage point change) non-parametric repeated two-samples test to compare outcomes between intervention and control groups before and after intervention. The changes in the dependent variable in the intervention group (from baseline to end line) were compared to the changes in the control group (from baseline to the endline). The intervention effect was measured by the odds ratio and 95% confidence level of the interaction term between study groups (intervention and control) and period of study (baseline and the endline) in the multivariate logistic regression model by adjusting the possible confounding variables. The Generalized Estimation Equation (GEE) was applied in addition to allow correlations of these repeated observations over time since data are collected on the same participants across successive points in time. A p < 0.05 was considered statistically significant.
link
More Stories
Nutrition during pregnancy: Healthy recommendations
Addressing the gaps in nutritional care before and during pregnancy | Proceedings of the Nutrition Society
Sorry, expectant moms: ‘Eating for two’ isn’t really a thing